The Health Communication Capacity Collaborative (HC3) team in Guinea is working with the communities hardest hit by the Ebola outbreak to rebuild both trust in the health system and the quality of care received. HC3’s approach incorporates evidence-based Social and Behavior Change Communication (SBCC), capacity-building and quality-improvement interventions.
In collaboration with Jhpiego and the Ministry of Health, HC3 is revamping a quality brand—entitled “Etoile d’Or,” or Gold Star—that will be promoted nationally and regionally through a mass-media campaign that includes radio, television, billboards and community events. The campaign aims to build confidence in as well as increase the use of health services.
Since 2012, Jhpiego has identified and assisted health facilities to meet quality criteria for service through a months-long accreditation process. Once accredited, a health facility receives a “gold star,” which is prominently displayed both inside and outside the facility. Currently, 15 facilities across the country have already received a gold star and another 22 are undergoing the accreditation process. Unfortunately, few people within these communities or health facilities understand the significance of the gold star label. That’s where HC3 comes in.
The first step in developing the new brand was to create an updated logo and campaign slogan that embody the values that community members think are most important when considering whether or not to use their local health services. These characteristics include: a health worker’s warm welcome, confidence, empathy, availability, respect and confidentiality as well as health facility cleanliness. The new logo is a gold star with a photo of two smiling male and female Guinean nurses inside, along with the slogan, “High quality services, your health is guaranteed!”
Once the logo and slogan are validated by all partners, new health facility signs, billboards, posters, and radio and television spots will be produced and distributed to promote the brand at the national and regional levels. Each community that already has a Gold Star facility will celebrate the campaign by unveiling the new logo at a community-wide launch party featuring speeches, theater and music.
By promoting the brand nationally, HC3 hopes to inspire non-Gold Star facilities to strive to achieve the same high-quality standards that Guineans desire and deserve. The Gold Star Quality Services promotion will encourage people to return to the life-saving health-care services that they stopped using during the time of Ebola.
https://ebolacommunicationnetwork.org/wp-content/uploads/2016/01/Etoile-dOr-logo_12-18-15.png30483048Hannah Mills | Program Officer | Johns Hopkins Center for Communication Programshttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngHannah Mills | Program Officer | Johns Hopkins Center for Communication Programs2016-01-19 09:54:512021-07-06 14:17:13After Ebola, Promoting New ‘Gold Star’ Brand to Increase Use of Health Services
The resurgence of Ebola in Liberia in late June 2015, seven weeks after the country had been declared Ebola free, put a spotlight on how the disease is transmitted, and brought the issue of sexual transmission to the forefront. With this shift away from coping with a national health emergency to dealing with what may now be a “new normal,” different public health messages are required for the people of Liberia.
Staff of the Ebola Survivors Clinic at work, Redemption Hospital in Monrovia. Image: WHO/C. Bailey
While new targeted behavior campaigns are being crafted, Liberians will have many questions about when and how Ebola is sexually transmitted. Journalists on the ground will need to find ways to tell that story.
There are helpful linkages to be found in HIV storytelling, but local media will need to address the fact that, unlike HIV-AIDS, the science on sexual transmission risk in Ebola is incomplete.
Ebola is both a sexually transmitted infection (STI) and not one. These stories should not provoke fear, but should communicate the need for safe sex.
“Through viral sequencing we are trying to establish the mode of transmission of the most recent (November) cases. Just as in July, we are also looking to see if it was the same viral strain present in Liberia in 2014”, says Tolbert Nyenswah, the Head of Liberia’s Incident Management System (IMS). “Of course, sexual transmission is a possibility in both cases,” he added.
Nyenswah is a co-author of a New England Journal of Medicine (NEMJ) article titled Molecular Evidence of Sexual Transmission of Ebola Virus, which reports on the examination of semen and vaginal-secretion samples collected from survivors in Liberia in March and April 2015. The case report describes one case of human-to-human EBOV transmission through sexual contact.
A pilot study, also published in the NEMJ, Ebola RNA Persistence in Semen of Ebola Virus Disease Survivors showed Ebola is able to live longer in the testes than previously known. Among the samples, Ebola virus RNA was detected in the semen of 11 of 43 (26%) men 7 to 9 months after the onset of disease. The authors recommend that the risk of sexual transmission of the Ebola virus should be further investigated.
Columbia University epidemiologist Stephen Morse was quoted in a “Popular Science” article,Why testicles are the perfect hiding spot for Ebola saying that he hoped the large numbers (of survivors) will make it easier to figure out when it’s safe for Ebola survivors to return to a normal sex life. “People may want to have children–they may have lost children, and want to go back to normal as soon as possible,” said Morse.
This is one of the questions researchers hope to answer in a National Institutes of Health studyinvolving more than 7,000 people who survived Ebola in Liberia for up to five years as they investigate the long-term health effects of Ebola virus disease. Researchers will seek to determine how survivors can still transmit the virus; also whether those they infect will present with Ebola symptoms and if survivors are at risk for illness in the future.
Though messaging guides during the West African Ebola epidemic all made reference to the possibility of sexual transmission – via bodily fluids – recommendations for changing sexual practices were not a priority for communications during the height of the crisis.
Rania Elessawi, Communications for Development Specialist at UNICEF in Liberia says during the days of the dying all normal human interaction just paused. No kissing, no hugging. What happens in people’s private lives was not even talked about. “Ebola changed the way we loved,” said Elessawi.
The success of the Ebola response, Elessawi says, was that people kept learning as the epidemic unfolded, and kept adjusting and changing the behavior change communications strategy, too.
The epidemic is now at a phase of much less handling and touching of patients and dead bodies in medical settings and at funerals where Ebola virus, present in bodily fluids, had been the primary mode of transmission.
“Now, the focus in behavior change messaging must shift to the realities of sexual transmission”, says Nyenswah of Liberia’s Incident Management System (IMS).
The UNICEF messaging guide for Ebola puts it this way:
Ebola survivors do not have Ebola, but it might be possible that Ebola can spread through doing man and woman business even after testing Ebola free. To make sure Ebola Survivors protect the people they love, they must use a condom correctly every time they do man and woman business. Make sure the survivor throws the used condom into the toilet or burn it.
For now, the WHO (interim) advice on the sexual transmission of the Ebola virus disease includes this guidance:
Until such time as their semen has twice tested negative for Ebola, survivors should practise good hand and personal hygiene by immediately and thoroughly washing with soap and water after any physical contact with semen, including after masturbation. During this period used condoms should be handled safely, and safely disposed of, so as to prevent contact with seminal fluids.
All survivors, their partners and families should be shown respect, dignity and compassion.
These two pieces of advice alone indicate the complexity and intimacy of communications and education around Ebola.
Community councillors doing education outreach with Ebola survivors, about combatting stigma. André Smith/Internews
Even with this new emphasis on human-to-human transmission through sexual contact, the question of Ebola’s origins refuses to go away. As before, during the height of the crisis, journalists will need to do their best to answer it.
Communicating the Complex Science of Ebola’s Origins to Shed Light on Human Transmission
The viral detective story in Liberia (as told in Part 1 of the PLOS post) has helped us understand more about the chain of human to human infections than has ever been known about Ebola, but, for many, the original question: “where does Ebola come from?” remains of concern. In other words, how exactly does zoonotic transmission – the chain of viral transmission from animals to humans – work?
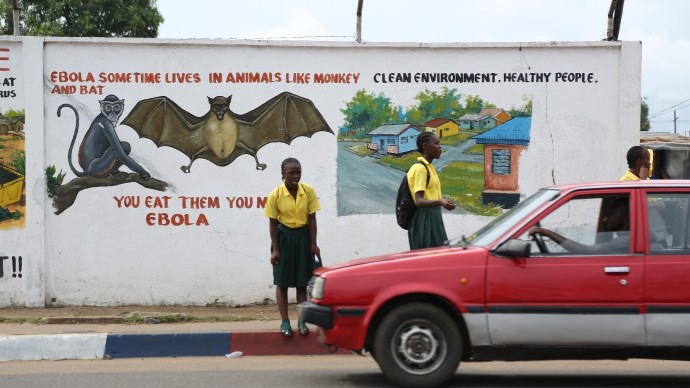
Warnings about the animal to human “jump” of Ebola, Monrovia. Image credit: André Smith/Internews
There has been no shortage of attempts to come up with answers.
Karl Johnson, former head of the Viral Special Pathogens Branch at the US Centers for Disease Control (CDC), interviewed for a July 2015 article in National Geographic, said that “despite arduous efforts by some intrepid scientists, Ebola virus has never been tracked to its source in the wild.”
And yet there is a widespread popular assumption – in Africa and elsewhere — that fruit bats were the source for the latest Ebola outbreak.
A 2005 article in Nature, titled “Fruit Bats as Reservoirs of Ebola virus” is the primary source for assertions that the Ebola virus resides in fruit bats, even though the authors made it clear their findings were inconclusive. Robert Swanepoel (now retired) who headed up the Special Pathogens Unit at the National Institute for Communicable Diseases in Johannesburg showed the virus survived in a single spider and in an insect eating bat. But Swanepoel is quick to add that his findings were proof of principle This means the study’s experimental approach – injecting Ebola virus into a range of plant and animal species, then testing if it would take hold – provided a strong signal that bats could be reservoir hosts but it was unable to draw conclusive evidence. The gold standard in science would be to be able to grow the virus in the lab from the viral fragments found in fruit bats.
Screening those samples back at his lab in Johannesburg, Swanepoel found no evidence of Ebola. So he tried an experimental approach, one that seemed almost maniacally thorough. Working in NICD’s high-containment suite—biosafety level 4 (BSL-4), the highest—he personally injected live Ebola virus from the Kikwit outbreak in 1995 into 24 kinds of plants and 19 kinds of animals, ranging from spiders and millipedes to lizards, birds, mice, and bats, and then monitored their condition over time. Though Ebola failed to take hold in most of the organisms, a low level of the virus—which had survived but probably hadn’t replicated—was detected in a single spider, and bats sustained Ebola virus infection for at least 12 days. One of those bats was a fruit bat.
“Journalists have to resist the temptation to oversimplify the complex and to provide answers where only theories exist”, says Jon Cohen, a staff writer for Science. “Pinpointing the origin of emerging diseases is a tricky business. A frightened public logically wants to know where a virus came from to protect people. But all too often, scientists only have clues — in the case of Ebola, bats seem like a logical source, and the first known case played in a tree that harbored bats.”
A WHO Fact sheet describes multiple possible animal sources for the transmission of Ebola to humans:
Ebola is introduced into the human population through close contact with the blood, secretions, organs or other bodily fluids of infected animals such as chimpanzees, gorillas, fruit bats, monkeys, forest antelope and porcupines found ill or dead or in the rainforest.
The Skoll Global Threats Fund hopes to create awareness and solutions around this transmission chain and the fact that “humans and animals increasingly share virulent viruses due to loss of green belts, global warming and poverty, raising the risk of highly disruptive pandemics.”
In simple language: it is widely accepted that there appears to be a link between the threatened habitats of chimpanzees and our shared susceptibility to Ebola. Fruit bats could be agents in spreading the virus from chimpanzee to chimpanzee, to other wildlife populations and perhaps even to humans.
Information Tools for Liberian Journalists
In an attempt to help journalists answer the question “where does Ebola come from?” Internews asked WHO veterinarian and epidemiologist Dr Maarten Hoek to explain this science to a group of environmental journalists in Liberia. He methodically took the journalists through Evolution 101, explained why and how diseases “jump” species and how it happens with greater ease if those species are closely related. He explained how the majority of diseases known to man are zoonoses, i.e. they jump from animals to successfully infect humans, reproduce and then transmit human-to-human. Ancient examples are tape worm, malaria and the common cold. HIV, SARS and MERS are more recent examples, and they jumped from chimps, bats and camels respectively.
One journalist in the Internews training told Hoek plainly: “As an environmental journalist I believe it, but as a person, I don’t. We have always eaten bush meat and bats. The forest has been there and is still there. Where does this Ebola really come from?”
Indeed, the Liberian landscape is lush forest, a sea of green. The valleys and gorges do not appear denuded to the naked eye.
In response to such skepticism, Dr. Hoek pointed to evidence of the decline in the quality and diversity of forest ecosystems. Further, he explains, improved roads and infrastructure are the blessing and curse of development. Whereas a viral infection such as HIV, might have flourished and remained in remote villages, killing all its hosts, our greater connectivity transports both humans and diseases near and far.
An “over-engineered” Liberian road. Image credit: André Smith/Internews
A World Bank 2010 report indicates about a third of Liberia’s roads are over-engineered relative to traffic levels. And, the 2014-15 West African Ebola outbreak demonstrated how quickly Ebola could spread once it reached urban centers.
In PLOS Neglected Tropical Diseases, Kathleen Alexander and colleagues provide a comprehensive outline of the interplay of dynamics that contributed to the Ebola outbreak in an article titled What Factors Might Have Led to the Emergence of Ebola in West Africa? A key dynamic discussed was the spillover of the virus to humans from wildlife – with bats as likely carriers. They also quote evidence that in West Africa, human movement is considered a particular characteristic of the region, with migration rates exceeding movement in the rest of the world by more than seven-fold. Solid science, but it still doesn’t make this story – as it relates to Ebola – easy to tell.
Monrovia, Liberia. Image credit: André Smith/Internews
I asked Jon Cohen of Science for advice on how Liberian journalists might tackle these complexities.“Our job is to tell it like it is, nothing more”. Cohen says as long as journalists explain – in simple language – that with Ebola, analysis of the viral genetic material gives it a fingerprint of sorts that links it to Ebola viruses seen earlier in the Democratic Republic of Congo.
“We know that viruses frequently pass from bats to humans, and there are documented cases of Marburg, Ebola’s close relative, likely infecting people who went into caves inhabited by Marburg-infected bats. We also have a documented case of Ebola moving from a dead chimpanzee to a human who handled the animal”.
Where is Ebola going?
Where is our understanding of the virus taking us? In a simple phrase: to more questions, more inquiry. There are more than 13,000 survivors across the three most affected countries in West Africa: Guinea, Liberia, and Sierra Leone. Scientists, the journalists who report the science and the communities affected are set to learn much more about the long-lasting effects of Ebola virus disease. And with this comes better insights on how to care for Ebola survivors, who strain from ongoing health problems. Many experience stigma, causing them to live in shame and fear. In an effort to prevent another Ebola crisis, the scientific community is working on developing an Ebola vaccine, of which they are cautiously optimistic, as is evident from current scientific discussion. See alsohttp://www.who.int/mediacentre/news/releases/2015/effective-ebola-vaccine/en/
Reporters in West Africa have been learning on the move, whilst living through a most devastating health emergency. Some have been in personal danger; many have been a truth link for their audience, separating gossip from genuine Ebola news. They have had to learn a whole new Ebola science lexicon, and have navigated reportage about issues that span death, dread, confusion, hope and aid politics. It’s too early to say that the dust has settled. But there has been time to think through the stories of the aftermath, to consider how Ebola has exposed the failings in the health system in Liberia and other West African countries – and what needs to be done to address that.
Moses Geply, an Internews trainee journalist in Liberia who is in the Local Voices journalism network, says he and colleagues are ready for this next phase of journalism that makes meaning of what happened in their country.
“This was a first-time health emergency for Liberia, so the mantra was: people won’t understand about this virus, how it spreads, and the medicines used to counteract it”, says Anahi Iacucci of Internews. “But what we learnt here is that really, it is not that difficult to transform a complex matter into something simple, you just really need to work very hard and find the right way to do it.”
Ebola is not over until it’s over. It may never be over. And we are just beginning to learn how to report on Ebola – including answering difficult questions about the origins of this disease.
Now the journalists living and working in Liberia need to make meaning of these new insights for their audiences. Not just the facts, but also what these facts mean – for the sake of their own safety, for their ongoing sense-making of this new and devastating disease.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/12/SurvivorTalk1_e-e1449575067948.jpg388690Ida Jooste | Global Health Advisor | Internewshttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngIda Jooste | Global Health Advisor | Internews2015-12-08 22:01:262021-11-11 15:11:09The Sexual Transmission of Ebola: Scicomm as a matter of life and death – Part 2 of 2
When I was in Liberia in June this year, just one month after the country had been declared “Ebola-free,” I noticed how often I heard the phrase “that was before Ebola” or “that was after Ebola”. The Ebola outbreak that began in 2014 brought unspeakable horror to a country still rebuilding after the war. News of new cases in late June 2015 again catapulted the country into high alert. In September 2015, the country was once more declared Ebola-free, but not for long. Ebola’s return in mid-November 2015 has produced yet another high alert.
Thus the realization is growing that it is not “before Ebola” or “after Ebola”, it is during Ebola. Ebola is with us, with the people of West Africa.
Before the 2014-25 Ebola outbreak that took 11,000 West African lives and made Ebola a worldwide concern, people in Liberia spoke of an event being “before the war” or “after the war.” Liberians lived through two conflict periods, the First Liberian Civil (1989 – 1996) and the Second Liberian Civil War (1999–2003). “References to before the war and after the war is a heuristic that individuals use to frame or situate the horrors of the war and what it entails. What might be unspeakable”, says Dr. Janice Cooper, who heads up the Carter Center in Monrovia’s mental health program. “It is a reference to which we can collectively relate”.
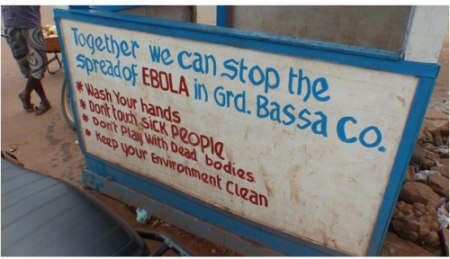
Billboards in Kakata in Margibi County, Liberia, where new Ebola cases were recorded in June and July 2015.
When Ebola re-emerged in Liberia in late June 2015, there were no panicked scenes, no people collapsing in the streets. According to the Dec. 2nd 2015 WHO situation report, a monthly case tracker, the June/July outbreak was confined to six cases. But the euphoria and pride Liberians felt at having defeated the disease was over. In its place, new questions emerged about what it all meant.
Translating Complexity
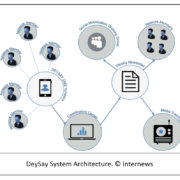
At Internews, a media development organization, where I serve as Global Health Media Advisor, we had navigated this complexity alongside local Liberia-based journalists for whom we provide training to help them respond to the Ebola crisis – and who then go on to produce their reports in various media, most often working on a shoestring. We also partnered with the humanitarian community to provide two-way communication channels to affected communities. Early in 2015, Internews set up DeySay, a rumor tracker that detects and manages Ebola-related rumors, which are coordinated and analysed for trends at a central hub in Monrovia. The tracker has picked up on wild speculation that the government of Liberia was profiteering from Ebola and recorded widely held beliefs that the disease is not real. Distrust in government is rooted in the years of civil war and conflict preceding Ebola. Also, early on in the outbreak, many people resisted treatment for Ebola because early presentation of the disease is with symptoms similar to malaria or even flu. Malaria is endemic in Liberia, and so often the (Ebola) symptoms seemed like those of a familiar disease.
“We would analyse the rumor and say: what’s the piece of information that is missing here? Where is the misunderstanding coming from? And then we provide that piece of information to our journalists and social mobilizers and religious leaders on the ground. It’s about really understanding where it’s coming from,” says Anahi Iacucci, Internews Senior Innovation Advisor, who led the Information Saves Lives project in Liberia and deployed DeySay.
In this way, DeySay has been a valuable journalistic tool used by Liberia-based reporters in the Internews training program. As rumors were collected with the DeySay tracker, myths were debunked by providing a factual correction or explanation as illustrated below:
Rumor from Sinoe County: There are people who are refusing to take their children to the hospital for the Polio and vitamin A immunization campaign because they believe that the government is using the campaign as a way to infect people with Ebola.
Well-sourced and accurate response: From the 26 nation-wide Polio and vitamin A immunization campaign: Children below the age of 5 were given free drops in the mouth to protect them from the polio virus. The polio immunization campaign was not organized by the government to infect people with the Ebola virus. With the vaccination, young children are protected against the virus, to ensure that Liberia will continue to be polio free.
Rumor from Nimba County: A woman in Nimba County was arrested after she refused health workers trying to give her child the Polio and vitamin A vaccine. She said the vaccine would infect the child with the Ebola virus.
Well-sourced and accurate response: A parent has the right to refuse the immunization of his child. No one should be arrested for refusing to take part in the immunization campaign.
Beyond tracking rumors, Internews is also partnered with GeoPoll in a project that traces the most frequently asked questions around Ebola. During all phases of the crisis – during Ebola’s peak in July to October 2014, in the Ebola-free phase as well as after its resurgence in July 2015 – the most enduring question has been: Where does Ebola come from?
The Medical Forensics of Ebola
Like the people of Liberia, scientists have also been asking this question; specifically, where did the new Ebola cases in Liberia come from, in late June, seven weeks after the country had been declared Ebola free, and again, in mid-November, ten weeks after the country had again been declared Ebola free. Although their present focus is on West Africa, the question of where Ebola originated has bedeviled virologists since the virus was first identified in 1976. In time this strain would be dubbed Zaire virus. Subsequently, additional strains of the virus emerged, named for the areas where they occurred. Later in 1976, Sudan virus was identified, a strain of the virus with a lower fatality rate than Zaire virus. Ivory Coast Ebola virus, isolated in 1994, showed slightly different characteristics again. In the period 1989–2007, three additional Ebola subtypes have been identified, Reston virus, Taï Forest virus and Bundibugyo virus. The strain of the virus present in the multiple outbreaks in West Africa since March 2014 is simply called Ebola virus.
So, where did the new cases in June 2015 come from?
A simple headline, released by Liberia’s Ministry of Health and Social Welfare, sums up a complex scientific investigation.
“Ebola virus genomes from latest flare-up rule out introduction from Guinea or Sierra Leone.”
The government’s news release further outlines the players and medical forensics that led to this conclusion:
“A joint team – including the Liberian Institute for Biomedical Research (LIBR), the United States Army Medical Research Institute for Infectious Diseases (USAMRIID) and the Liberian Ministry of Health – has sequenced the EBOV isolated from the index case in this cluster.”
As Tolbert Nyenswah, the Head of Liberia’s Incident Management System (IMS) later explained, “The form of the virus present in June was of a mutation present in Liberia, not neighboring countries. Both sequences are identical and are consistent with this cluster representing a continuation of the EBOV outbreak in Western Africa, as opposed to a separate introduction from a reservoir population.”
Say What?
Through-out the epidemic, viral sequencing had shown different mutations of the current strain found in West Africa, thus enabling scientists to identify the origin of a single infection as being a version circulating in localized parts of Liberia, Sierra Leone or Guinea. This resolution of the Ebola DNA detective story helped put an end to the common rumor that the new Ebola cases came from across the border, from Guinea or Sierra Leone. Or did it? As the science on Ebola has unfolded, those most affected have been trying to make sense of the complex procedures utilized in scientific laboratories to arrive at such conclusions. However, this language is not easy to follow if you’re new to molecular genetics. So, the question local journalists repeatedly faced was How can we make sure this critical information is broadly understood by the people?
Internews trainee Eric Opa Doue of Echo Radio, which provides Ebola news in Rive Cess County, Liberia. Photo by: Andre Smith/Internews
“This news is in deep science, not in English,” says Eric Opa Doue, a community radio journalist in the Internews health training program who holds a degree from the Ghana School of Journalism.
“I first need to digest and simplify it, then send it to the translation department at my station, to ensure the message is correctly deciphered in Kru and Bassa languages for my audience, so that everyone will understand. For example, Opa Doue asks, “what does the following sentence (from the Liberian government’s news release) mean – in plain language:
‘The sequence groups closely with previous isolates from Liberia and is distinct from the viruses currently circulating in Sierra Leona and Guinea.’”
Most importantly, local Internews reports focused on the fact that this scientific finding ruled out cross-border transmission from Sierra Leone or Guinea. It also ruled out rumors, including that the boy died from eating infected dog meat. In essence, the message became the fact that this was the same Ebola they’d been dealing with since 2014.
“Ebola Deeply”
Ebola Deeply, an independent global digital media project led by journalists and technologists whose goal is to “build a better user experience of the story by adding context to content,” also took on this challenge. Work such as their two-part series Unlocking Ebola’s Secrets has been helpful to Internews trainees and others following and attempting to explain this story. To produce this report, the Ebola Deeply team visited Liberia’s genome sequencing center where researchers examined the genome of viral samples taken from the 17-year old boy who died in the town of Smell no Taste in Margibi County. There they learned that by using genome sequencing, the scientists were able to determine that the viral strain in the boy’s body was genetically similar to that circulating in this area of Liberia last year. The viral forensics had shown that the virus which killed the 17-year-old young man in June 2015 and which caused Ebola to re-emergence in a small pocket in his town in Margibi County, had the same signature as the virus present in his area earlier in 2015.
As the Ebola Deeply journalists explained in Unlocking Ebola’s Secrets, the process of genome sequencing is like “turning the pages of the virus’s personal diary”.
Learning (More) from Ebola
Toward the end of July 2015, the WHO’s Dr Bruce Aylward and colleagues from the US Centers for Disease Control and the Liberian Ministry of Health told humanitarians responding to the Ebola crisis that the world of science is braced for a period of immense learning. The West African Ebola epidemic has been the most devastating the world has seen. More than 11,000 people have died, and, connected to this scale and to an increasingly more efficient Ebola response, is the fact that this epidemic has left behind the largest number of Ebola survivors ever – people who have been infected, but who did not die of Ebola. To families, these are loved ones who are still with them; to science, this is an opportunity to unravel some of the many questions about Ebola that remain unanswered.
What scientists like Aylward are now saying about Ebola are things that could not have been tackled in the horror and haste of the humanitarian crisis, when the entire focus was about saving lives and preventing transmission to caregivers from those who were dying.
In part two, I discuss what is being learned about new modes of Ebola virus transmission and the public health messages that are being prepared and implemented to communicate the implications for the people of Liberia.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/12/EricSign_P1040600_e-e1449501625616.png389690Ida Jooste | Global Health Advisor | Internewshttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngIda Jooste | Global Health Advisor | Internews2015-12-07 15:23:322021-06-23 10:18:22Where Does Ebola Come From? Communicating Science as a Matter of Life and Death – Part 1 of 2
Ebola affected every Sierra Leonean in or out of the country. It altered our planned activities at work, as we could no longer travel upcountry. My children sat painfully at home for more that a year when they should have been learning in school. We lost families and friends. Yes, Ebola has not only changed me, but it changed our culture. I no longer do handshakes or hugs. I am not as keen as I was in the past to attend funerals. I insist that my family always carry hand sanitizers.
Sierra Leone President Ernest Bai Koroma. Photo credit: Dauda Musa Bangura
Now that outbreak has been declared over, for those of us here, one thing rings true: “we are all survivors.”
Sierra Leone recorded the first case of Ebola on May 24, 2014 and the World Health Organization (WHO) declared the country free of Ebola on November 7, 2015, after going 42 days without new cases. This milestone resulted in widespread jubilation. Already the streets are lined with wedding cars, and so much gathering here and there. The end of Ebola is so timely as it ushers in the Christmas holidays and the New Year. We have felt deprived for almost two years and everyone I know has determined to enjoy themselves well.
But some Sierra Leoneans are approaching the news with caution. Speaking at an official declaration ceremony on November 7 at the Bintumani Hotel in the capital city of Freetown, Yusuf Kamara, a healthcare worker and an Ebola survivor who lost 16 members of his family, lamented, “for us, Ebola is not over.” He appealed to Sierra Leone President Ernest Bai Koroma and his development partners to address “the many, many health problems we still suffer from.”
For his part, President Koroma thanked the 35,000 Ebola response workers and honored all those who died. “I am here today as your Head of State to tell you that collectively we have prevailed over this evil virus,” he said. He declared November 18 as National Ebola Day, and revealed that November 21, 2015 will be a national day of thanksgiving.
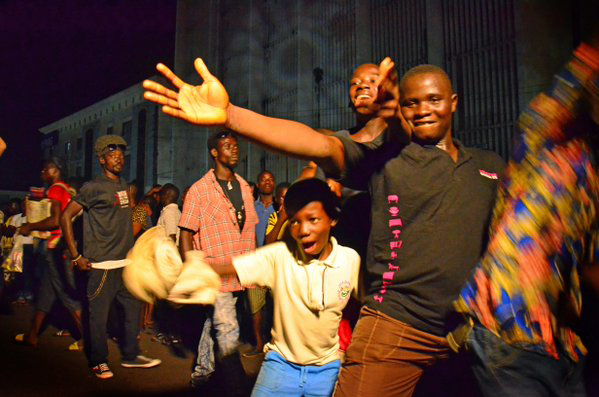
Sierra Leoneans celebrating to mark the 42 days of no new Ebola infections. Photo credit: Dauda Musa Bangura
As the Government of Sierra Leone was making their celebration, many others where doing their own bit: the traditional and religious leaders, women’s movement, the “Okada” boys (association of motorbike riders), the entertainment industry, private sector, and international and national development partners. It was a rainbow moment for Sierra Leone. Everyone had a reason, or otherwise found a reason to celebrate. They paid tribute to the dead, saluted the brave health care workers, hailed the burial teams, made heroes of the survivors and celebrated the sacrifices that they made to bring the virus to a halt.
At a jam-packed candlelight vigil organized by the women of Sierra Leone on November 6, the names of all the health workers who lost their lives to Ebola were read out and awards given to some key partners who fought the “war.” Words cannot describe the anxiety held across all of the nation’s 14 affected districts during the last week leading to the declaration. In a mournful tone, Fatmata Katta, a Program Officer with the Health Communication Capacity Collaborative (HC3) project Sierra Leone tried, saying, “it’s been a tough week,“ adding, “I teared each time I listened to the reflections on the radio.”
For Maseray Foray, a 15-year-old student at Waterloo Street in Freetown, she was happy for the stigmatization to stop. “I did not get Ebola, but I got the treatment and I can only imagine what our survivors are going through,” she said, explaining her experience with immigration when trying to visit another West African country. “Today is the happiest day of my life as I would no longer be seen as a virus,” she said.
According to WHO, a total of 8,704 people in Sierra Leone were infected during the outbreak. Some 3,800 people survived and 3,589 died. From those who sadly lost their lives, 221 of them were healthcare workers including 11 doctors. They were all remembered and honored vividly during the many celebrations that took place across the nation on this day.
Candlelight vigil. Photo credit: Dauda Musa Bangura
This outbreak highlighted the critical role that social and behavior change communication (SBCC) plays in containing transmission. Reflecting on the emergency response in a working paper titled, “The Ebola Response in West Africa ODI,” a question was raised about the consequences of not prioritizing SBCC early enough to contain the spread, as responders focused more on bio-medical interventions. “Given the scale of the outbreak and the vastly insufficient treatment facilities, should decreasing transmission through behavioral change (rather than through case isolation) have played a dominant role?” The article went on to quote Claudia Evers, an Emergency Coordinator of MSF, to say, “Instead of asking for more beds we should have been asking for more sensitization activities.”
The next 90 days remain crucial to ensure that the country remains at zero cases. The public is mandated to continue calling the emergency Ebola free hotline when a death occurs and for the swabbing of all bodies for testing before burials until mid-2016. The country’s economy was badly hit during this period and now has much more challenges to worry about. These include how to care for its survivors, the stigmatization they face and their many ailments including vision problems, fatigue, joint pain and depression and how to cater for its estimated 12,000 orphans and over 10,000 teenagers left pregnant during Ebola. Sierra Leone, however, owes the upscale of hand washing practices nationwide and the observation of infection prevention and control measures in health centers to the “unwelcome guest.”
Emma Vincent, Program Officer II, HC3 Sierra Leone Program. Photo credit: Dauda Musa Bangura
The country also remains vigilant of it its borders with neighboring Guinea, the source of the Ebola outbreak, which is still struggling to contain the disease. Meanwhile, Liberia was declared free of Ebola on September 3, 2015.
“Indeed it has been a joyous moment for us that at long last we can start to heave a deep sigh of relief from the outbreak, which has dealt a heavy blow on all aspects of our lives,” said Sierra Leonean Reverend Alimamy Kargbo. “But we will never never give up.”
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/12/ebola-free-sierra-leone-celebration.png397599Emma Vincent |Program Officer II | HC3 Sierra Leone Programhttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngEmma Vincent |Program Officer II | HC3 Sierra Leone Program2015-12-01 15:24:112021-11-11 15:16:14After Reaching 42 Days with No Ebola Cases, One Thing Rings True for Sierra Leoneans: “We are all Survivors”
In July 2015, three months after the last person who had succumbed to the dreadful Ebola virus was buried, Liberians woke to the news that a 17-year old young man had died of the virus. Liberia was no longer considered Ebola-free.
Franklin D. Roosevelt’s words, “The only thing to fear is fear itself” have stayed with me since the first news stories broke about the Ebola outbreak in West Africa, quickly followed by stories of chaos and fear. As someone who has worked with and in the media, I also know that lack of accurate information is a big driver of fear and trauma, which in turn can easily translate into stigma and a withholding of sympathy for those affected by the traumatic events, driven by a compulsion to exclude them as “other.”
It’s been well documented that the Ebola crisis was in large part driven by misinformation in the early days of the outbreak. Rumors spread quickly, and massive blasts of communication, which although aimed at helping people understand the disease and how to deal with it, often ended up being contradictory and just plain confusing. Everyone knew that accurate Ebola information was critical. However, what was missed in the scramble to communicate, was listening to the people affected by the crisis. Simply booming messages at people affected by a crisis is bound to fail.
Internews, a specialized partner of the Health Communication Capacity Collaborative (HC3), found more than “300 types of social mobilization and messaging systems in the three worst-affected countries: Liberia, Guinea and Sierra Leone.” As the organization’s Senior Director for Global Initiatives Alison Campbell described it: A “chaotic information landscape [that] consisted mainly of information ‘out’ with little opportunity for community dialogue.”
Internews has vast experience working in humanitarian disasters, so it was a natural fit to partner with HC3 already working in Liberia, to widen the approach to getting lifesaving messages to people knowing full well that in rapid onset epidemics, rumors can kill. Who better to target than local journalists deeply connected with their own communities? Whichever way you look at it, individuals need to know the facts and the science behind the disease they’re covering in the media. Working with Liberian journalists was therefore key to Internews’ approach to ensure people had access not only to a wide range of information from trusted sources, but also to channels for questioning and discussing that information.
Alison summarized five takeaways earlier this year in an article that she thought the international development community should take to heart.
Form genuine partnerships with local media.
Build capacity rather than paying to disseminate prepared messages.
Deliver consistent messages and don’t oversimplify.
Encourage two-way communication with community audiences.
Help local media realize their full potential as a platform for accountability.
Internews’ health journalism advisor, Ida Jooste recently visited HC3 in Liberia. She spoke to me about how working with journalists can address the stigma related to Ebola. She also shared some insights into Internews’ partnership with HC3, which showed that the commitment and community engagement has been sustained, despite the assumption that there may be Ebola fatigue or messaging fatigue. Community radio journalists have continued to be actively involved in Ebola-related programming in a way that shows “they care and are deeply committed to their communities,” Ida noted. “By investing in groups and journalists who had already proactively taken leadership in the Ebola response, the HC3/Internews team merely added a multiplier effect.”
IDA:Internews in Liberia provides training and follow-up mentoring to a select group of journalists, including from counties most affected by Ebola. These five-day training workshops provide journalists with resources and discussion points of the Ebola-related issues that dominate the news agenda in Liberia. Apart from the obvious joy of the country having been declared “Ebola free” by the WHO on 9 May, the most pertinent discussions relate to:
The fact that neighbouring countries still have Ebola cases; and
Stigma against survivors and survivors’ integration into society.
In the week of 25 May, Internews held a weeklong workshop with main theme: Mental health and Ebola. The group was addressed by Dr. Janice Cooper, The Carter Center’s Country Representative, who leads the Center’s Liberia Mental Health Initiative. In the Ebola crisis, she is bringing her expertise in mental health issues to promote an understanding of depression and of the negative effects related to the “othering” of Ebola survivors. Dr. Cooper explained mental health issues themselves are stigmatized. Traditional beliefs hold that mental health-related issues are a curse or punishment from God. When Ebola survivors show signs of depression (most do), they and their surrounding community first need to understand the biological and mental processes behind depression and anxiety. Through adapting existing mental health approaches, she and her teams are helping survivors by teaching coping mechanisms. The Carter Center’s work also extends to creating acceptance and a supportive environment. Dr. Cooper gave an outline of her work to journalists, and introduced them to an Ebola survivor, who answered journalists’ questions about how they are feeling and how they are being treated.
Survivors typically experience self-stigma, guilt (because they survived and others didn’t or because they may have infected others); they are fearful of the recurrence of disease; they re-live the dread of having been so ill and of losing loved ones and they also may still be severely ill and fear that ongoing symptoms will not disappear or get worse. They are widely stigmatized, because some believe they must be bewitched or “the walking dead”, because they managed to survive a disease — around which the initial messaging had been “Ebola kills”! All of this information and accounts of these experiences were passed on to the journalists, who are planning to use the material in their radio talk shows, or radio, TV and print feature stories.
Internews also developed a Rumor Tracker (DeySay – a reference to how people speak about rumors in Liberia), which responds to rumors and debunks myths picked up through the extensive rumor tracking system. These (rumors and factual corrections) are then disseminated to partners through a humanitarian info newsletter, intended for dissemination amongst those who communicate with communities. “DeySay” uses dedicated outreach workers from local partner organizations, as well as local journalists who report rumors through SMS messages to a hotline, where these rumors are categorized by topic and regional scope. Sources include Facebook groups, hashtags on Twitter, influential bloggers, and local media including those from the diaspora, mapping online conversations and triangulating with SMS information from outreach workers. The Rumor Tracker’s information is then fed back to the community of social mobilizers, local media, public officials, and faith-based organizations, as well as to the international humanitarian community in a weekly newsletter that highlights trending issues by community or area. It identifies the most prevalent rumors, provides insights into local and social media coverage, and provides recommendations for addressing the information gaps identified.
Callie: How did this link to HC3’s social and behavior change communication campaign/messages?
IDA:HC3 has been responsive to the issue of most concern in Liberia, stigma against survivors and produced a comic book that communicates messages which helps integrate survivors into communities through normalizing behaviors. Internews distributes these comic books to trainee journalists as a resource. Billboards with the message, “Everyone is a survivor” are commonly seen in Monrovia and in counties. By aligning journalism training with the emerging issues in the country and the issues HC3 has identified as pertinent for its communications strategy, Internews training is responsive to the current information needs in the country.
Callie: How big a problem is stigma?
IDA:The survivors we spoke to, as well as those working in the mental health and counselling field, say it is a really huge problem. Apart from the stigma issues highlighted above, survivors also face the stigma of poverty. In many cases, harvests could not take place because of Ebola. All “Ebola households” were destroyed, meaning sick people and their families lost everything they owned. The belief that survivors benefitted with huge cash payouts does not help their plight. These are all issues that communicators and journalists are working to address.
When you take these factors into account, it is clear why combatting stigma is such an important aspect of Internews’ and HC3’s overall response. More than working to change behavior related to the frightening disease, what needed to happen was to work with communities to tackle the fear and associated stigma that cast such a deadly pall.
For other Internews-related work in Liberia using radio to stem an epidemic, click here.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/08/Internews-Ebola-Aug2015.png798978Brandon Desideriohttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngBrandon Desiderio2015-08-19 16:56:432021-11-11 15:15:38Fighting Fear and Stigma with Accurate Ebola Information
It’s a win for Ebola prevention efforts that over 120 people in Liberia were placed under observation due to a resurgent outbreak in the country, even after it was declared Ebola-free. This signals that Liberia’s containment efforts are still strong. But it’s essential to remain vigilant: as the epidemic wanes, public complacency around sustaining behaviors that prevent Ebola transmission could be a barrier to stemming the flow of new cases for good.
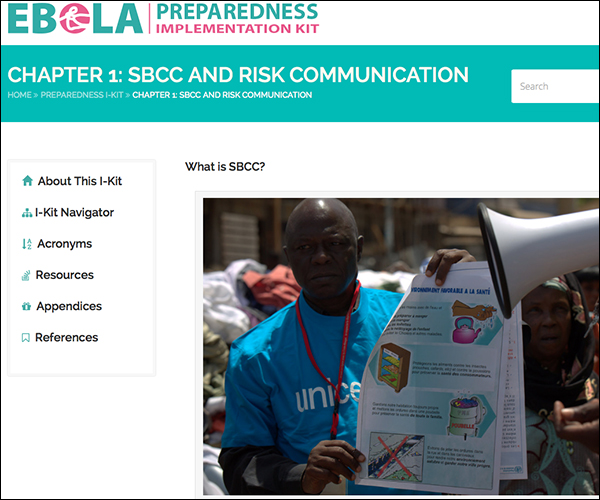
This new Ebola Preparedness Implementation Kit (I-Kit) explains that all emergencies evolve in phases, as do emergency communication efforts. The Ebola outbreak is in Stage 4 of emergency communication: Resolution. Reported new cases have decreased significantly, SBCC interventions are well underway and regular informing of the public is ongoing. We’re certainly on “the Road to Zero,” and sustaining momentum so that preventative behaviors like hand-washing remain the status quo is crucial for actually getting there.
In the I-Kit, we outline creating a centralized mechanism for Ebola communication response, focusing on social mobilization and media/communication coordinating mechanisms; we also provide guidance on developing an Ebola communication strategy with step-by-step illustrative examples.
Some of the most helpful features in the I-Kit are interactive, like our Checklist for putting a communication coordinating mechanism in place. The I-Kit’s appendices are also rich with resources, like a conceptual framework for control and prevention of Ebola, and an overview of the relevant health communication theories put explicitly into the Ebola communication context.
We encourage you to explore our Ebola Preparedness I-Kit and to pass it along. Headlines in the West may have shifted the public’s focus away from Ebola—but the global response is far from over.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/07/ebola-preparedness-i-kit-image.jpg500600Brandon Desideriohttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngBrandon Desiderio2015-07-23 16:11:052021-11-11 15:14:58As Ebola Epidemic Wanes, Transform Complacency with this Ebola Preparedness I-Kit
On May 22, the Health Communication Collaborative (HC3) will participate in a panel discussion on communication research and the Ebola response at the International Communication Association’s 65th Annual Conference in San Juan, Puerto Rico.
A teleconference line will be provided for those unable to attend in person. The panel will take place from 9:00 AM – 11:45 AM EDT.
The overall aim of the panel, “Communication Research Response to the Ebola Outbreak: The Only Cure Available,” is to reflect upon the recent outbreak and emphasize the importance of including health communication and culture in a response to rapidly emerging health threats. By providing critical, theoretical, and data-driven perspectives, the panelists will demonstrate the value and capability of communication theory and research in an outbreak.
Using a social ecological approach, the panel will discuss research focused on policy and culture, health systems, community and individual response, and how those areas are integrated. Key integration questions to be discussed include:
What can communication scholarship and practice reveal about public response to an emerging health issue like Ebola?
What does an emerging health issue like Ebola reveal about links between different domains of communication theory and praxis?
What can we learn from the communication response to Ebola that will move the field of health and development communication forward?
The Panel
Collins Airhihenbuwa – Head and Professor of Bio-behavioral health, The Pennsylvania State University
Catie Bailard and Silvio Waisbord – School of Media and Public Affairs, George Washington University
Michael Bailey and Amanda Berman – Johns Hopkins Center for Communication Programs
Daniel Barnett – Department of Environmental Health Sciences, Johns Hopkins Bloomberg School of Public Health
Maha Bashri – Department of Communication, Bradley University
Mohan Dutta – Provost Chair Professor and Head, Department of Communications and New Media, National University of Singapore
Maria Elena Figueroa – Department of Health Behavior & Society, Johns Hopkins Bloomberg School of Public Health
Maria Lapinski – Associate Dean for Research, College of Communication Arts and Sciences, Professor, Department of Communication and Michigan AgBio Research, Michigan State University
Rafael Obregon – Chief, Communication for Development Section, Gender, Rights and Civic Engagement Cluster Programme Division, UNICEF
Shaunak Sastry – Assistant Professor, Department of Communication University of Cincinnati
The Moderators
Douglas Storey – Director for Communication Science and Research, Center for Communication Programs, Johns Hopkins Bloomberg School of Public Health
Khadidiatou Ndiaye – Milken Institute School of Public Health, George Washington University
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/05/ica4.png250300Kathi Fox | HC3 Communications Associatehttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngKathi Fox | HC3 Communications Associate2015-05-19 17:20:092021-11-11 15:11:31Communication Research and the Response to Ebola: An ICA Panel May 21-25
Liberia’s Information Minister receives audio equipment from HC3’s Teah Doegmah.
The Health Communication Capacity Collaborative (HC3) has provided audio equipment to the Liberian Ministry of Information, Cultural Affairs and Tourism (MICAT) in Monrovia to help it improve its outreach to the public in case of another public health crisis such as Ebola.
“We are pleased to support MICAT and help in any way we can to improve communication and outreach to the Liberian people,” said Teah Doegmah, HC3’s Social and Behavior Change Communication Program Officer. “Especially in light of the Ebola outbreak last fall.”
The equipment, valued at close to $3,000, includes an audio mixer, audio cables, microphone stands, speakers, and a laptop. The equipment will be used for public addresses, including press briefings, and audio editing.
MICAT Minister Lewis G. Brown, who received the equipment, expressed his gratitude to HC3, which is a five-year global health communication project funded by USAID and based at Johns Hopkins Center for Communication Programs. HC3 has been active in the global response to Ebola by providing social and behavior change communication support in Liberia, Sierra Leone and Guinea.
Brown said the equipment will help MICAT provide important public health information to the public in a timely manner.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/04/TeahDoegmahMakingPresentation.png230384Kim Martinhttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngKim Martin2015-04-15 14:54:352021-08-31 15:13:33Liberia’s MICAT To Use Audio Equipment from HC3 for Public Health Outreach
Please join in a three-partwebinar seriesbeginning April 1
Health workers in West Africa have been responding to Ebola since 2013, and, according to the latest WHO situation report, the pace of the outbreak is beginning to decline. This calls for relief and celebration. However, this is far from final for those who have been affected by Ebola.
The virus has left indelible marks on their lives, and their stories are many and severe:
“The Ebola situation is once more improving in terms of infection rate, but the socio-economic needs are enormous.” (Moses Khanu, Pastor, Sierra Leone)
Health workers remain at the center of community response and support. At the same time, the governments and international organizations that support health workers are seeking answers for how they can restore health services in West Africa, strengthen health systems, and prepare for future health emergencies.
What’s next for Ebola affected countries?
Distributing fresh water to families; Photo credit: Moses Khanu
Many organizations are working closely with all actors across the health sector. What comes next for Guinea, Liberia and Sierra Leone, the three most affected countries? And how can countries nearby and in the region plan for future potentially deadly outbreaks? In the second series of Training Health Workers for Ebola webinars in April, a group of colleagues who have been working in the affected countries will talk about lessons learned and planning for rebuilding and strengthening health systems. Participants are invited to join in the discussion during the webinars.
Reviewing lessons learned, and looking ahead
These webinars will focus on tools and strategies that health workers, as well as the governments and organizations that support them, can use to continue the response, protect their communities and help rebuild health systems. Free training and information resources are concurrently being posted on the Ebola Resources for Health Workers website.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/03/Moses-Khanu-Photo-featured-image.png496900Marla Shaivitz | Health Communication Capacity Collaborativehttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngMarla Shaivitz | Health Communication Capacity Collaborative2015-03-30 15:18:262021-07-06 14:16:45Training Health Workers for Ebola Response and Community Support Webinar Series
‘Kick Ebola From Liberia’ is a weekly radio programme produced in Liberian English that launched last November. The show is broadcast across the country 112 times a week on more than 20 partner stations. Early on, our aim was to provide information and discussion about how to avoid catching the Ebola virus, obtaining early treatment, practicing safe burials and breaking the chains of transmission. But now that the crisis has entered a new phase, we are shifting our focus, addressing issues such as immunisations, livelihoods and education after Ebola.
The programme is produced by BBC Media Action, which has partnered with the Paul G. Allen Foundation to deliver communication training to media, officials and humanitarian workers in 10 countries at risk in Africa. The partnership includes producing media outputs – such as ‘Kick Ebola From Liberia’ and the mini-drama series Mr. Plan Plan – to help people take action to protect themselves and their communities in Liberia, Sierra Leone and Guinea.
For ‘Kick Ebola From Liberia,’ we work with a team of Liberian journalists to produce our stories. From individual tales of inspiration to serious interviews with government officials to in-depth stories about community-based solutions, we aim to address the issues that matter most, tackle rumors, and address issues of stigma. The focus is on discussion and collaboration, encouraging Liberians to band together and support each other through the crisis and into the immediate recovery phase. Listeners are invited to submit questions and contributions via text, Facebook and WhatsApp, which we incorporate into each the radio show.
https://ebolacommunicationnetwork.org/wp-content/uploads/2015/03/kickebolafromliberia.jpg480720Jenny Marchttps://ebolacommunicationnetwork.org/wp-content/uploads/2021/03/ebola-communication-network-lg-1030x363.pngJenny Marc2015-03-23 13:54:002021-07-28 16:20:54Radio Program “Kick Ebola From Liberia” Shifts Focus; Addresses Immunizations, Education





















{kind=link}